
Some thoughts from a healthcare perspective
“Safety culture” is something that many will have heard of. But what is safety culture? Is it important for actual safety outcomes? Or is it an entirely academic matter, with no relation to how things work in your organisation? Does having a positive culture make any difference in the real world?
These are important questions in many safety-critical sectors such as process, manufacturing industries, healthcare and social care. In this blogpost and two further posts, I will unpick some of the key questions and try to offer some insights you can apply in your own work.
In this post, we will talk about organisational culture generally and the link between safety culture and safer outcomes. Our second post looks at organisational maturity, its evaluation and what is really meant by a learning organisation. Finally, we look at how systems and culture affect the response to problems in the pharmaceutical sector including issues identified by the regulator which require corrective or preventative actions (CAPAs) – CAPA culture.
Organisational culture – the way we do it here?
It’s probably true to say that we will all have an intuitive perception of culture. Perhaps we think of it as its “character” or even its “personality”. When we move from one organisation to another, we’ll probably notice some differences. Perhaps some organisations are more open and welcome discussion. Some are instead more focused on achieving their immediate goals and seem to have little time to listen to staff.
There are many types of organisations and many characteristics. They may not be easy to define, but often they are simply recognised and experienced. So what does “culture” really mean? Here’s a starting point (though it’s not necessarily a complete or accurate description): organisational culture has often been summarised as “the way we do it here”, and as such is immediately obvious to staff.
But why does culture vary so much? Is it merely differences in behaviour (the way we do things here) or are there other factors in play? Most people who have studied this believe that behaviour isn’t the whole story and that the underlying attitudes, values, beliefs and assumptions in the organisation play a significant role in its culture.
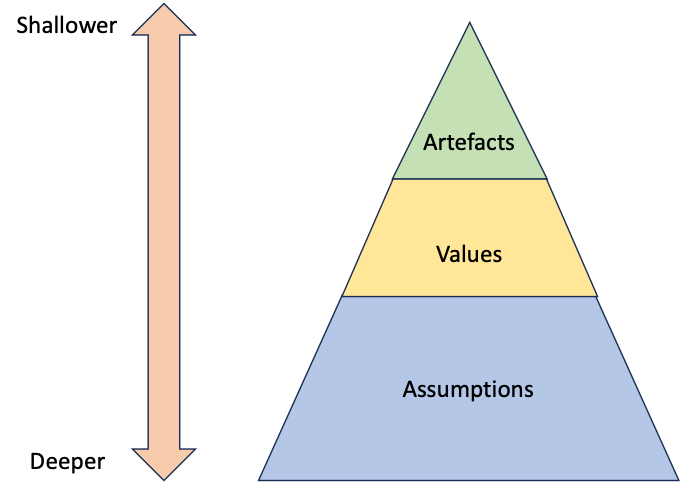
E H. Schein1 visualised organisational culture on three levels: artefacts – tangible, overt indicators that include uniforms, behaviours, language and even some systems such as how we report and investigate incidents. Values are said to be the “reasons and/or rationalizations for why members behave the way they do in an organization”. At the most fundamental and enduring level, Schein defined assumptions as “unconscious patterns that determine how group members perceive, think, and feel”.
It’s worth thinking for a moment about organisations that you are familiar with. What are the assumptions and values they espouse, and what would you point to as the artefacts you identify?
And how quickly can these change? Can we easily change the assumptions of the team, or more easily address way we do things?
What’s more, there isn’t a single culture in an organisation. In healthcare organisations, for example, there is sometimes a difference between the culture of managers, whose immediate responsibilities are to the structures and functioning of the organisation, and clinical staff, whose direct responsibilities are always to the patient.
Safety culture…
Safety Culture is a part of the overall culture of the organisation, and once again there are many definitions. For example, many people would say that safety culture is the way in which safety is managed in the workplace. It is the combination of beliefs, perceptions, and attitudes employees have toward safety. Sometimes the term “safety climate” is used to descibe the value placed on safety in an organisation at a particular point in time or a particular place, but the terms are often used interchangeably.
There are definitions, and there are tools to measure culture and discuss culture. And there are our own experiences of working in different cultures and with different teams – because even small teams have different characteristics and different values placed on safety and safe behaviours.
…or a culture of blame?
Okay – we can see that there’s this thing called safety culture but so what? We can probably see that it might affect our mood at work, say, or how we get along in the workplace – but does culture affect safety?
There’s a famous line from Peter Drucker which sets out the essence:
Culture eats strategy for breakfast
And in the UK National Health Service, for example, the Medical Director Sir Liam Donaldson emphasised in 2000:
‘Blame cultures’ … can encourage people to cover up errors for fear of retribution and act against the identification of the true causes of failure, because they focus heavily on individual actions and largely ignore the role of underlying systems. The culture of the NHS still errs too much towards the latter2.
Blame culture. Well, some readers will recognise the description only too well. I have heard staff in healthcare settings describe the general response to incidents that involved humans as “name, blame, shame and retrain”. Familiar? It will be to many workers, I’m quite sure!
Let’s look at this sector – healthcare – for a moment. There has been a great deal of research in this area, trying to answer the question “Is having a positive culture associated with positive patient outcomes?”
Within the body of research, perhaps our best guide on this issue is a meta-analysis3 (a review of as many relevant papers as possible that identifies consistent findings) carried out in many settings. Based on this work and our current understanding of its significance, it seems likely that having a positive culture is associated with positive outcomes for patients. Some of the outcomes the authors identified in this work are:
- Lower mortality
- Better management of the deteriorating patient
- Fewer adverse events and medication errors
- Fewer readmissions to hospital
And in hospitals, having a positive culture is also associated with better outcomes in the areas of:
- Patient falls
- Acquired infections (HAIs)
- Pressure ulcers
- Deep vein thromboses
Does it seem that safety culture is important? It certainly looks that way. Most members of staff will have experienced different cultures with different characteristics and will recognise how this subtle but pervasive quality affects their own wellbeing and the quality of work carried out. Positive cultures are associated with positive outcomes.
What does a safe culture look like?
Many researchers and workers in the field of organisational culture believe that culture is an “emergent property” of organisations. It is observable, but not understandable in terms of causal connections. Think of mixing blue and yellow paint and making green; green wasn’t there at all in the ingredients, but emerged as a property of the mixture. So the results of cultural surveys can tell us where we are but not how to change. It’s difficult stuff, culture!
| Safety culture components Culture is sometimes thought of as a “complex” phenomenon. That means it comprises many components and interactions and can’t be easily understood or predicted in the way a purely linear system can be. But when it comes to safety culture, we can try to find out how it can relate directly to how we can improve. Safety culture is linked to: • reporting culture: creating an organizational culture in which staff are prepared to report their errors or near-misses. • just culture: not a total absence of blame, but an atmosphere of trust in which people are encouraged to provide safety-related information – at the same time being clear about where the line is drawn between acceptable and unacceptable behaviours. • flexible culture: which respects the abilities of staff (especially those at the “sharp end”) and which allows control to pass to task experts on the spot; • learning culture: the willingness and competence to draw the appropriate conclusions from its safety information system, and the will to implement major reforms where their need is indicated4. |
But a critical aspect of safety culture relates to how it treats error. We know from systems thinking that error is more usefully seen as a consequence of the way we work rather than a cause of problems. When we understand that no-one comes to work to do a bad job, but that errors happen naturally in an imperfect system, blame becomes counter-productive. Telling people to be “more careful” or to “work harder” simply doesn’t work. And blaming people, instead of trying to understand why it made sense for them to act the way they did, only discourages them and their colleagues from disclosing errors.
In turn, that closes down channels of communication and therefore makes the system less safe. Instead, our organisations should be working towards a “Just Culture”.
Error, blame and justice
I mentioned “Just Culture” in Box 2. You might have heard of this, especially in healthcare, where it has been promoted by many healthcare organisations. A just culture considers wider systemic issues where things go wrong, enabling professionals and those operating the system to learn without fear of retribution.
In a just culture, inadvertent human error, freely admitted, is not normally subject to sanction, to encourage reporting of safety issues. In a just culture, investigators principally attempt to understand why failings occurred and how the system led to sub-optimal behaviours. Importantly, a just culture recognises the rare instances where issues of accountability are nevertheless appropriate to consider, so a just culture aims to hold people appropriately to account where there is evidence of gross negligence or deliberate acts.
Systematic tools can be used to distinguish intentional or negligent acts from systems-based issues of care. This tool is based on James Reason’s “Incident Decision Tree” and is available as the NHS “Just Culture Guide”5. Using the tool allows us to determine the influence of systems factors such as training, supervision, equipment and environment, and also to assess how other staff would have handled a difficult situation.
The just culture approach ensures a systematic way to identify systems factors after errors. In the rare circumstances where someone’s actions may have been inappropriate, it also supports a conversation about whether a staff member involved in a patient safety incident requires specific individual support or intervention to work safely.
Safety culture? Yes, there is a point
As more and more evidence accumulates to show the associations between safety culture and outcomes, we will need to evaluate and address culture more intelligently. Safety culture’s key qualities (Box 2) can be consciously addressed – when you know what your local culture is.
Perhaps the starting point for many organisations is reporting. Reporting is absolutely essential in identifying incidents that require a response, as well as in recording low impact incidents and “near-misses”. These give you a good handle on where future incidents might occur and where your organisation might have uncontrolled risks.
A reporting culture is a key element of a learning organisation – but it is not the only one. At Human Reliability Associates, we have developed a model of organisational learning that we have applied to many industries – healthcare, power generation, transport and heavy industry.
In the next blogpost, I will set out the elements of this model and relate it to the creation of a true learning organisation. You can use this to start to build an understanding of the maturity of your organisation with regard to safety. Is your organisation mostly proactive, for example – or is it bureaucratic, or even pathological?
Catch the next blogpost!
Dr Stephen Cross
Senior Associate Consultant, Human Reliability Associates
Dr Steve Cross and Professor Peter Spurgeon authored the NHS Patient Safety Syllabus and Curriculum Guidance at the Academy of Medical Royal Colleges on behalf of NHS England.
HRA offers human factors consultancy services to support Human Factors in the healthcare industry. To learn more about how we can support you, click here.
HRA previously played a leading role in supporting the Safety Clinical Systems initiative. To read more about the project, click here.
References
- Somers, M., 2023. 5 enduring management ideas from MIT Sloan’s Edgar Schein. [Online]
Available here. - Department of Health, 2000. An Organisation with a Memory. Available here.
- Braithwaite, J. et al., 2017. Association between organisational and workplace cultures, and patient outcomes: systematic review. BMJ Open, 7(:e017708), p. :e017708.
- Munro, E., 2008. A review of safety management literature, s.l.: Unpublished.
- NHS, n.d. A just culture guide. [Online]
Available here.

